The Medications Used in Dementia Care: What Each One Actually Does
An honest, plain-language guide to the medications used in Alzheimer's and dementia today — donepezil, memantine, the new amyloid-targeting antibodies (lecanemab and donanemab), and the medications used for behavioral symptoms. What each one does, what it doesn't, and what to watch for.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
The Medications Used in Dementia Care: What Each One Actually Does
If your parent has been diagnosed with Alzheimer's or another dementia, you will, sooner or later, sit in front of a doctor who is recommending medication. The doctor will talk about it for ten minutes. You will leave with a prescription, a printed handout, and a question you didn't quite get answered: what does this drug actually do?
This post is an honest, plain-language guide to the medications used in dementia care today. We'll cover what each one is for, what it actually does (and doesn't do), and what to watch for. Before we start: none of these medications cure dementia. None of them stop the disease. The most we can say is that some slow it modestly, some help with symptoms, and one new class can clear the abnormal proteins in the brain. Understanding the difference between those is what this post is for.
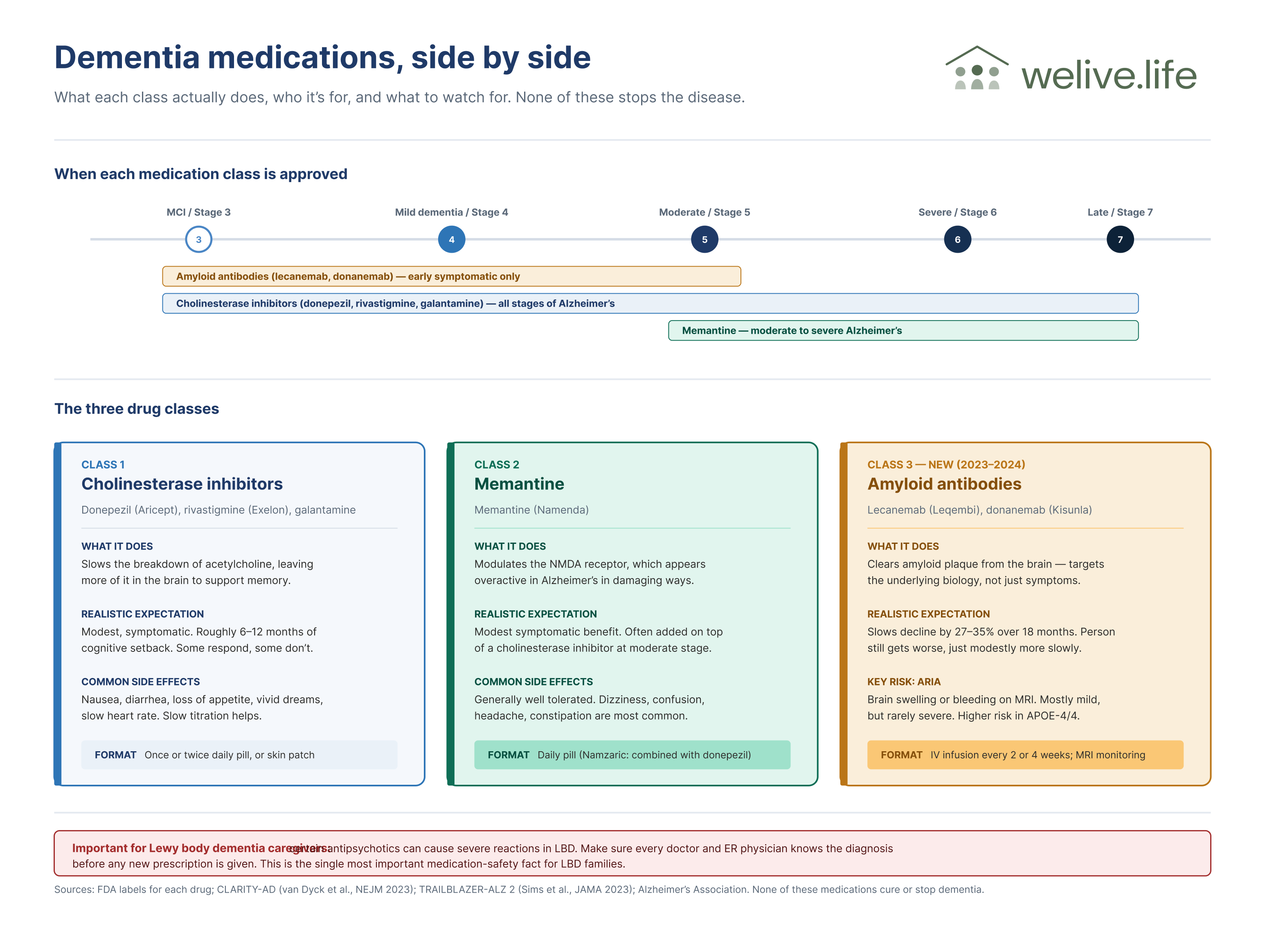
The two main classes of cognitive drugs
For decades, the only medications available for Alzheimer's disease worked by adjusting brain chemistry rather than addressing the underlying disease. They are still the most-prescribed dementia drugs today.
These three drugs all work in roughly the same way. In Alzheimer's disease, the brain progressively loses neurons that produce acetylcholine, a chemical messenger involved in memory and learning. Cholinesterase inhibitors slow the breakdown of the acetylcholine that remains, leaving more of it available in the synapses.1
The effect is symptomatic — the drugs do not slow the underlying disease. They make the brain a little more efficient with what's left. In clinical practice, the benefit is modest: studies show small but measurable improvements in cognition and daily function, typically equivalent to setting back the clock on cognitive decline by about six to twelve months.1 Some people respond noticeably; some don't respond at all. There is no reliable way to predict in advance who will benefit most.
Donepezil (Aricept) — once-daily pill. Approved for all stages of Alzheimer's. The most commonly prescribed.
Rivastigmine (Exelon) — available as a pill or skin patch. The patch is often easier on the stomach.
Galantamine (Razadyne) — twice-daily pill. Less commonly prescribed today than donepezil.
The most common side effects are gastrointestinal — nausea, diarrhea, loss of appetite — particularly when starting or increasing the dose. Slow titration helps. Other side effects include muscle cramps, vivid dreams, and slow heart rate. Anyone with a history of bradycardia or certain heart-rhythm conditions should make sure their cardiologist is in the loop.
NMDA receptor antagonist: memantine
Memantine (Namenda) works through a different mechanism: it modulates the activity of the NMDA receptor, which appears to be over-stimulated in Alzheimer's in ways that damage neurons.1 Memantine is approved for moderate to severe Alzheimer's, often added on top of a cholinesterase inhibitor in mid- to late-stage disease.
The benefit, again, is modest and symptomatic. Memantine is generally well-tolerated. The most common side effects are dizziness, confusion, headache, and constipation.
A combination drug, Namzaric, packages donepezil and memantine in a single capsule. It's convenient but typically more expensive than the two component drugs taken separately.
The new class: amyloid-targeting antibodies
Beginning in 2023, the FDA approved a new class of drugs that work very differently. Instead of adjusting brain chemistry, these drugs target one of the underlying biological hallmarks of Alzheimer's: the buildup of amyloid plaques. They are infused intravenously, and they clear amyloid out of the brain.
This is a genuinely new chapter in dementia treatment. It is also a chapter that requires careful expectation-setting, because the magnitude of clinical benefit is real but small, and the risks are real and not small.
Lecanemab (Leqembi)
Lecanemab received full FDA approval in July 2023.2 It is approved for early symptomatic Alzheimer's disease — meaning mild cognitive impairment due to Alzheimer's or mild dementia from Alzheimer's — with confirmed brain amyloid pathology.
In the CLARITY-AD phase 3 trial, lecanemab slowed clinical decline by approximately 27% over 18 months compared to placebo, as measured on the CDR-Sum of Boxes scale.3 In practical terms, that's a difference of roughly five months of disease progression over a year and a half. People taking lecanemab still got worse — they got worse a bit more slowly.
The drug is given as an IV infusion every two weeks. It requires confirmed amyloid pathology (via PET scan or CSF biomarkers) before starting, and ongoing MRI monitoring during treatment.
Donanemab (Kisunla)
Donanemab received full FDA approval in July 2024.4 It is approved for the same population — early symptomatic Alzheimer's with confirmed amyloid plaques.
In the TRAILBLAZER-ALZ 2 trial, donanemab slowed clinical decline by approximately 35% in the low-to-medium tau subgroup over 18 months, measured on the iADRS scale.5 Like lecanemab, the magnitude of benefit is meaningful but not transformative — measured in months of slowed decline, not in disease arrest.
Donanemab is given as a monthly IV infusion. A distinctive feature: in the trial, treatment could be stopped once amyloid had been cleared from the brain to a defined threshold, raising the possibility of a finite course of treatment rather than indefinite dosing.
The risks: ARIA
Both lecanemab and donanemab carry a risk of amyloid-related imaging abnormalities, abbreviated ARIA. This is the part of the conversation that often gets compressed in the doctor's appointment.
ARIA comes in two forms: ARIA-E, which is brain swelling, and ARIA-H, which is small areas of bleeding in the brain. Most cases are detected on MRI before causing symptoms, and most are mild and resolve on their own. But some cases are serious. In the trials, a small number of patients had severe events including symptomatic brain hemorrhage and, in rare cases, death.35
The risk is meaningfully higher in people who carry two copies of the APOE-4 gene — and in those people, the FDA labels carry specific warnings.2 Anyone considering an amyloid antibody should have APOE genotyping done first, and the doctor should walk through what the result means for their personal risk.
Who should consider amyloid antibodies, and who shouldn't
These drugs are approved for early Alzheimer's only. People in moderate or severe stages of dementia were not studied and are not eligible. People with significant cardiovascular risk, prior stroke, certain anticoagulant use, or substantial existing amyloid-related changes on baseline MRI are typically not candidates.
The decision to start one of these drugs is not straightforward. The benefit is real but small. The risk is real but manageable for most people. The cost — even with insurance — can be substantial. The infusion schedule is demanding. The MRI monitoring is intensive. For some families, those tradeoffs make sense; for others, they don't. There is no wrong answer.
Medications for behavioral symptoms
As dementia progresses, behavioral and psychological symptoms — agitation, anxiety, depression, sleep disturbance, hallucinations — often emerge. Several classes of medication can help.
Antidepressants, particularly SSRIs like sertraline and citalopram, are sometimes used for depression and anxiety in dementia. They are generally well-tolerated and can also help with agitation.
Antipsychotics — including risperidone, olanzapine, and quetiapine — are sometimes used off-label for severe agitation, aggression, or psychosis. They carry an FDA black-box warning about increased mortality risk in older adults with dementia, and should be used at the lowest effective dose for the shortest necessary period.1 In Lewy body dementia, certain antipsychotics can cause severe and dangerous reactions and should generally be avoided.
Brexpiprazole (Rexulti) received FDA approval in 2023 specifically for agitation associated with Alzheimer's disease — the first drug to receive that specific indication. It is an antipsychotic, and it carries the same class warnings as the others.
Sleep, anxiety, and pain medications are also sometimes used cautiously. The general rule in dementia is to start very low, go very slow, and revisit any medication whose benefit isn't obvious.
What to ask your doctor
Before starting any dementia medication, useful questions include:
What is this drug actually expected to do for my parent? Symptomatic improvement, disease modification, or behavior management?
How will we know if it's working? What's the timeline before we should expect to see (or not see) benefit?
What side effects are most common, and which are serious enough to call you about?
Are there interactions with my parent's other medications?
For amyloid antibodies specifically: has my parent had APOE genotyping? What does the result mean for their personal ARIA risk?
If we don't see benefit, when would we consider stopping?
The goal of dementia medication is to extend good time, manage symptoms, and slow decline where possible. None of these drugs can stop the disease. Knowing what they actually do — and what they don't — is the foundation for using them well.
— King
References
Alzheimer's Association. "Medications for Memory, Cognition and Dementia-Related Behaviors." 2024. alz.org
U.S. Food and Drug Administration. "FDA Converts Novel Alzheimer's Disease Treatment to Traditional Approval." July 2023. fda.gov
van Dyck CH, Swanson CJ, Aisen P, et al. "Lecanemab in Early Alzheimer's Disease." New England Journal of Medicine 2023;388:9-21. NEJM
U.S. Food and Drug Administration. "FDA Approves Treatment for Adults with Alzheimer's Disease." July 2024.
Sims JR, Zimmer JA, Evans CD, et al. "Donanemab in Early Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial." JAMA 2023;330(6):512-527.
.png)