A founder's guide to the genetics of Alzheimer's — what APOE-4 means, what one copy versus two copies actually changes, the difference between APOE-4 and the deterministic genes, and the GINA insurance gap every family should know about before testing.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
The Genetics of Alzheimer's: What APOE-4 Actually Means for Your Family
I have a personal stake in this topic. After watching my mom go through Alzheimer's, I wanted to know whether I carried the gene variant that had likely shaped her disease — APOE-4. I carry one copy of e4 and one copy of e3. That genotype puts me at higher risk than baseline, but not at the very high risk of someone with two e4 copies. It was useful information.
Getting that information was harder than it should have been. This was years ago, before consumer genetic testing was as easy as it is now. I started by doing deep research to understand the science — what APOE-4 actually does, what one copy versus two copies meant, and crucially, whether there was anything I could do about it if the answer came back unfavorable. Once I'd convinced myself that the answer to that last question was yes, I went looking for ways to find out my own genotype. I ended up uploading my raw genetic data into a third-party tool to get the answer, because the clinical pathway for APOE testing was narrow.
Today, you don't have to do any of that. Genetic testing is widely available through clinical labs, and APOE genotyping specifically is straightforward to request. This post is the guide I wish I'd had when I started — what APOE actually is, what one or two copies of the e4 variant means for your odds of Alzheimer's, the difference between APOE-4 (a risk gene) and the rare deterministic genes that cause early-onset autosomal-dominant Alzheimer's, the practical question of whether to get tested, and the things — like long-term-care insurance — that families should think about before they do.
The science here moved in 2024, and the post reflects that. Specifically, there's now strong evidence that carrying two copies of APOE-4 isn't merely a "risk factor" in the usual sense — it functions more like a distinct genetic form of Alzheimer's disease. That finding is the most important update in this field in years, and we'll cover it.
What APOE actually is
APOE — apolipoprotein E — is a gene that codes for a protein involved in transporting cholesterol and other fats in the body and the brain. Everyone has two copies of the APOE gene, one inherited from each parent. The gene comes in three common variants, called alleles: e2, e3, and e4.1
e3 is the most common variant. About 60% of people carry two copies. It is considered the "neutral" baseline.
e2 is less common and appears to be modestly protective against Alzheimer's.
e4 is the variant associated with increased Alzheimer's risk.
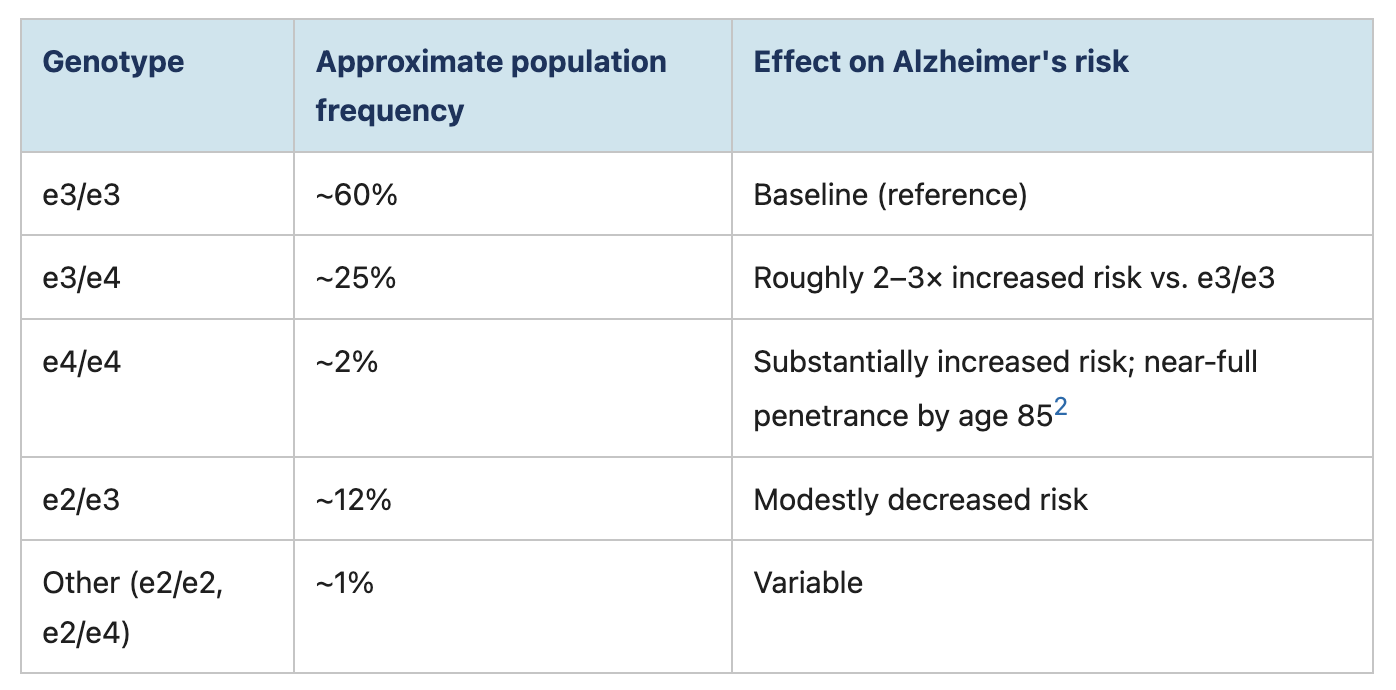
Because everyone has two copies of the gene, you can have any combination of these alleles. The combinations are called genotypes:
What the 2024 research showed about carrying two e4 copies
For decades, APOE-4 was described as a risk factor — a variant that raised your odds of developing Alzheimer's but did not guarantee it. That description is still accurate for people with one copy. But for people with two copies, a 2024 paper in Nature Medicine by Fortea and colleagues argued that the term "risk factor" understates what's happening biologically.2
The researchers analyzed clinical and biomarker data from over 3,000 brain donors and 10,000 individuals. They found that by age 65, nearly all APOE-4 homozygotes (people with two copies) had abnormal amyloid biomarkers in their cerebrospinal fluid, and 75% had positive amyloid PET scans. The age of symptom onset was earlier and more predictable than in non-carriers — typically 7 to 10 years earlier. The pattern, in short, looked more like the deterministic forms of Alzheimer's than like a typical risk factor.
The authors concluded that APOE-4 homozygosity should be considered a distinct genetic form of Alzheimer's disease, not merely a risk factor. The National Institute on Aging summarized the finding the same way.3
For families with a homozygous APOE-4 carrier, this matters. It means that planning for the disease is more reasonable than betting against it.
The deterministic genes: APP, PSEN1, PSEN2
APOE-4 is by far the most common high-risk gene for Alzheimer's. But there is a separate category of genes that cause Alzheimer's outright, in a pattern called autosomal dominant inheritance. If you carry one of these mutations, you will almost certainly develop the disease, typically before age 65.4
The three known deterministic genes are:
APP (amyloid precursor protein) on chromosome 21
PSEN1 (presenilin 1) on chromosome 14
PSEN2 (presenilin 2) on chromosome 1
Together, mutations in these three genes account for less than 1% of all Alzheimer's cases worldwide. They are most relevant in families with multiple cases of early-onset Alzheimer's across generations — typically diagnosed in the 30s, 40s, or 50s. If your family fits that pattern, genetic counseling and testing for these deterministic genes is a separate conversation from APOE-4 testing, and an important one.
Should you get tested?
This is the question that brings most people to this kind of post. There is no universally right answer.
The case for testing:
You want to know your risk so you can make informed decisions about lifestyle, planning, and personal priorities. The evidence from large prevention trials like FINGER and U.S. POINTER is strong that lifestyle interventions matter, and they may matter more for people at higher genetic risk.
You're considering whether to enroll in clinical trials of preventive therapies. Some trials are open only to people with specific APOE genotypes.
You're considering an amyloid-targeting antibody (lecanemab or donanemab) — APOE genotyping is required, because the risk of ARIA is meaningfully higher in APOE-4 homozygotes.
You want to plan financially, professionally, and personally for the possibility of disease, while you have the time and capacity to do so.
The case against:
A positive result cannot tell you when, or even if for sure, you will develop Alzheimer's. The information has limits.
It can affect insurance — particularly long-term-care insurance and life insurance, which are not protected by federal anti-discrimination law (more on this below).
For some people, the psychological burden of a positive result outweighs the practical benefit of knowing.
If you do decide to get tested, the gold standard is to do it through a genetic counselor or a physician, not through a consumer DTC product alone. A genetic counselor can help you think through whether testing is right for you, can explain the results in context, and can help you decide what to do with them.
The insurance issue every family should know about
The Genetic Information Nondiscrimination Act of 2008 (GINA) prohibits health insurers and employers from using genetic information to make coverage or hiring decisions.5 That's the good news.
The less-discussed news: GINA does not apply to:
Life insurance
Long-term-care insurance
Disability insurance
This is a significant gap. If you take a genetic test that reveals APOE-4 status — whether through a clinical lab or a consumer service — and you later apply for long-term-care insurance, the insurer can ask whether you've had genetic testing, and they can use the result.
The practical implication: if you are considering long-term-care insurance, talk to a broker about your options before you get tested. Some families decide to lock in coverage first.
What APOE-4 carriers can actually do
If you find out you carry APOE-4 — particularly two copies — the most important thing to understand is that the result is information, not a sentence. Lifestyle factors continue to matter. The 2024 Lancet Commission identified 14 modifiable risk factors that account for an estimated 45% of dementia risk globally.6 The 2025 results from the U.S. POINTER trial showed that a structured lifestyle intervention — combining exercise, nutrition, cognitive challenge, social engagement, and cardiovascular health — improved cognition over two years, and the effect held across APOE genotypes.7
For APOE-4 carriers, that last detail is important. The intervention worked even in people at higher genetic risk. Genetics is not destiny.
The practical things that appear to matter most, based on current evidence:
Aerobic and resistance exercise on a regular schedule
None of these are dramatic. Most are things doctors have been telling people to do for years. The new research is what they reduce dementia risk by — and for APOE-4 carriers, the absolute benefit is meaningful.
A note from someone who's been through this
The order I went through this in mattered more than I realized at the time. I researched the science before I tested. By the time I had my own genotype in hand — one e4 copy, one e3 — I already understood what the result would and wouldn't tell me, and I'd already convinced myself that the lifestyle work was worth doing regardless of the answer. That meant the result became a calibration, not a verdict. It told me roughly how much risk I was carrying compared to baseline, and it sharpened my commitment to the things that move the needle. It didn't tell me my future.
If you're thinking about testing and you're not sure, do the research first. Read about what APOE-4 actually means. Talk to a genetic counselor. Decide what you would do differently with the information before you have it. Then, if testing still makes sense to you, the result is much easier to sit with — whether it comes back e3/e3, e3/e4, or e4/e4.
— King
References
National Institute on Aging. "Alzheimer's Disease Genetics Fact Sheet." 2024. nia.nih.gov
Fortea J, Pegueroles J, Alcolea D, et al. "APOE4 homozygozity represents a distinct genetic form of Alzheimer's disease." Nature Medicine 2024;30(5):1284-1291. Nature Medicine
National Institute on Aging. "Study defines major genetic form of Alzheimer's disease." May 2024. nia.nih.gov
Alzheimer's Association. "Genetic Testing for Alzheimer's Disease." 2024. alz.org
National Human Genome Research Institute. "Genetic Information Nondiscrimination Act (GINA)." 2024. genome.gov
Livingston G, Huntley J, Liu KY, et al. "Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission." The Lancet 2024;404(10452):572-628. The Lancet
Baker LD, Snyder HM, Espeland MA, et al. "Structured vs Self-Guided Multidomain Lifestyle Interventions for Global Cognitive Function: The U.S. POINTER Randomized Clinical Trial." JAMA 2025. JAMA
.png)